



Posterior tibial tendon dysfunction (PTTD) is one of the leading causes of adult-acquired flatfoot. There is often delay in the identification of this condition until foot deformation and changes in mobility have already occurred. It occurs due to a defect in the posterior tibial tendon.
PTTD can affect anyone but is more frequently seen in women over 40 years of age. Individuals with obesity, diabetes, hypertension, rheumatoid arthritis, or a history of ankle injuries can also develop this disease. Medical experts recently identified PTTD is not restricted to a single tendon involvement. Rather it involves the entire arch support system including the tendons, ligaments, and bones. This identification led to the renaming of PTTD to Progressive collapsing foot deformity (PCFD)
This article discusses posterior tibial tendon dysfunction in detail, including its causes, symptoms, stages, diagnosis, treatment options, rehabilitation exercises, recovery timelines, and strategies to prevent progression and maintain long-term foot function.
What is PTTD?
Posterior tibial tendon dysfunction (PTTD), also called Progressive collapsing foot deformity (PCFD) occurs when the posterior tibial tendon flexible band of tissue which (connects muscles to bone) becomes inflamed, weakened, or damaged , losing its ability to support the arch of the foot.
The posterior tibial tendon (flexible band of tissue which connects muscles to bone) connects the calf muscles to several bones on the inside of the foot. It plays an important role in supporting the foot's arch, maintaining balance, and helping movements such as walking, running, climbing stairs, and standing on tiptoes. This results in:
- The loss of support from the posterior tibial tendon causes the foot to gradually flatten and roll inward.
- This leads to the progressive flattening of the foot of the arch thereby causing an acquired flat foot or fallen arch.
- Over time, this may lead to pain, difficulty walking, and progressive deformity of the foot and ankle.
- In the more advanced stages there is the involvement of the surrounding ligaments, joints, and bones.
Early diagnosis and treatment are important to relieve symptoms, prevent worsening of the deformity, and improve long-term foot function.
Who Is at Risk for PTTD?
Posterior tibial tendon dysfunction can affect anyone. It is most commonly seen in women over the age of 40. Certain medical conditions, lifestyle factors, and foot mechanics can place additional stress on the posterior tibial tendon, increasing the likelihood of tendon degeneration and arch collapse.
Risk factors for PTTD include:

People with any of the above risk factors who have additional symptoms of pain or swelling on the inner side of the ankle should consult their Doctors to rule out PTTD.
What Causes PTTD?
PTTD develops when the posterior tibial tendon is unable to withstand the stress and forces placed upon it, leading to its inflammation, degeneration, or tearing. Common causes of PTTD include:
- Overuse and repetitive stress: Physical activities such as running, hiking, climbing stairs, or standing for long periods can mechanically overload (put excessive stress or force placed on a tendon, muscle, bone, or joint beyond what it can safely tolerate) the tendon. With time this repetitive overloading exceeds beyond the tendon's natural capacity to heal, leading to gradual structural breakdown and loss of proper function
- Overpronation or flat feet: Excessive inward rolling of the foot (Overpronation) increases strain on the posterior tibial tendon, making it work harder for arch stability. People with already existing flat feet are more likely to develop PTTD as their posterior tibial tendon is already under strain to maintain arch stability.
- Acute injuries: An ankle sprain, fall, or direct trauma to the foot can injure the posterior tibial tendon and damage its structure and function. At the same time, previous injury could hamper the blood supply and structure of the tendon.
- Age-related degeneration: Tendons lose elasticity and strength with age, increasing the risk of PTTD, particularly after the age of 40.
- Obesity: Excess body weight places increased stress on the feet and tendons during weight-bearing activities. The long term overloading increases breakdown, weakens the tendon's structure, and increases the risk of dysfunction
- Inflammatory conditions: Diseases such as rheumatoid arthritis can weaken the tendon and surrounding structures, impair tendon healing, and progressively reduce the proper functioning of the posterior tibial tendon.
- Chronic medical conditions: Diabetes mellitus and hypertension have been associated with an increased risk of tendon breakdown. Diabetes reduces collagen synthesis and hypertension causes reduced blood supply to the tendon.
- Long term steroid exposure: Repeated steroid injections or long-term steroid use may weaken tendon tissue and increase the likelihood of tendon rupture.
PTTD Symptoms
Symptoms of PTTD initially might be mild but they gradually worsen with its progression.
In early stages symptoms include:
- Pain in the inner ankle which is throbbing or aching in nature and worsens on activities like walking, climbing stairs and running.
- Mild swelling
- Tenderness along the tendon
- Tiredness while walking
As the condition progresses, patients may notice:

Stages of Posterior Tibial Tendon Dysfunction (PTTD)
Posterior tibial tendon dysfunction (PTTD) is a progressive condition that is commonly classified into four stages based on the severity of tendon damage, foot deformity, and ankle involvement.
Stage I
At this stage, the posterior tibial tendon is inflamed but remains intact and functional. The foot maintains a normal shape, and the foot arch has not collapsed in this stage.
Symptoms include:
- Pain and tenderness along the inside of the ankle and foot
- Mild swelling over the tendon
- Pain that worsens after prolonged walking, running, or standing
- Ability to perform a single-leg heel raise, although it may be painful
Treatment:
This stage responds well to conservative treatment, including rest, activity modification, immobilization, orthotics, physical therapy, and anti-inflammatory medications.
Stage II
In Stage II, the tendon becomes elongated and weakened, reducing its ability to support the arch. The foot begins to flatten, but the deformity remains flexible, meaning that it can still be manually corrected by a healthcare professional.
Symptoms include:
- Progressive flattening of the arch
- Pain along the inside of the ankle
- Difficulty or inability to perform a single-leg heel raise
- Positive "too many toes" sign, where more toes are visible from behind because the forefoot has drifted outward
- Pain while walking long distances or standing for prolonged periods
Treatment:
Many patients can still be treated successfully with braces, custom orthotics, physical therapy, and activity modification. Surgery may be considered if conservative treatment fails.
Stage III
At this stage, the flatfoot deformity becomes rigid and can no longer be manually corrected. Arthritis often develops in the joints of the hindfoot.
Symptoms include:
- Constant pain that may extend from the inside to the outer side of the ankle
- Severe flattening of the foot
- Joint stiffness and reduced foot mobility
- Difficulty walking
- Pain on the outer side of the foot caused by the collapsed arch, which allows the heel bone to press against the outer ankle (subfibular impingement)
Treatment:
Because the deformity is rigid, surgical reconstruction or joint fusion is often recommended.
Stage IV
In Stage IV, the deformity progresses to involve the ankle joint, leading to instability and arthritis. The supporting ligament on the inside of the ankle (deltoid ligament) may also become weakened.
Symptoms include:

Treatment:
Treatment often involves complex reconstructive procedures or ankle and hindfoot fusion surgery, depending on the severity of joint damage.
Stages of Posterior Tibial Tendon Dysfunction (PTTD), Common Symptoms, and Treatment Options.
| Stage | Symptoms | Treatment |
|---|---|---|
| Stage I | Pain and swelling along the inside of the ankle, tenderness over the posterior tibial tendon, pain after walking or running, normal foot arch, and a painful but possible single-leg heel raise. | Rest, activity modification, walking boot or brace, anti-inflammatory medication, custom orthotics, and physical therapy. |
| Stage II | Flattening of the arch, flexible flatfoot, positive "too many toes" sign, difficulty or inability to perform a single-leg heel raise, and pain during prolonged walking or standing. | Custom orthotics or an ankle-foot brace, physical therapy, strengthening exercises, activity modification, and surgery if conservative treatment fails. |
| Stage III | Rigid flatfoot deformity, constant pain, pain on the outer side of the ankle due to bone impingement, severe arch collapse, joint stiffness, and difficulty walking. | Surgical reconstruction or joint fusion is often recommended to relieve pain and correct the deformity. |
| Stage IV | Severe flatfoot with ankle involvement, ankle instability, arthritis, chronic pain, and significant difficulty walking and performing daily activities. | Complex reconstructive surgery, ankle stabilization procedures, or ankle and hindfoot fusion, depending on the severity of joint damage. |
When to See a Doctor for PTTD?
If you suspect any of the following symptoms it is best to visit your doctor for early identification and treatment:
- Pain on inner ankle side
- Progressive flattening of foot arch
- swelling along the inside of the ankle that does not improve with rest.
- Find it difficult to walk, stand, or climb stairs because of foot pain.
- Cannot stand on your tiptoes on the affected foot.
- Notice your foot is rolling inward or your heel is tilting outward.
How Is PTTD Diagnosed?
Diagnosis of PTTD involves detailed clinical examination, radiographic evaluation and advanced imaging.
Clinical Examination: First doctors assess the
- Foot alignment
- Walking pattern
- Ability to raise the heels
- Tendon tenderness
- Too many toes sign
X-rays: Assess bone alignment of the foot region.
Ultrasound: Identifies tendon tears and damage
MRI: Shows degeneration and inflammation of tendons .
CT Scan: Useful in advanced deformities.
Treatment of PTTD
The treatment of PTTD depends upon the stage in which the patient comes to the doctor. Early stages can be managed by conservative treatment while advanced cases require surgery. It is advised to visit your doctor as soon as possible if you suspect PTTD because early diagnosis improves the chances of recovery.
Conservative Treatment (Stages I and II)
When detected early PTTD can be managed conservatively without the need for surgery. The steps of conservative treatment include:
1. Activity Modification
- The main aim is to avoid activities that over load the tendon.
- High-impact activities like running, basketball, and jumping should be reduced or avoided temporarily.
- Low-impact activities like swimming, cycling, and water aerobics, which maintain fitness without straining the tendon are advised.
2. Short-Term Immobilization
Doctors might suggest walking boots or CAM walkers for 3–4 weeks can allow initial tendon healing. These are specialized supporting aid which remove the pressure from the tendon and allow its recovery.
3. Orthotics and Bracing
Custom foot orthotics (insoles):
- Shoe inserts that support the arch, improve foot alignment, and reduce strain on the injured tendon.
- Best for Stage I. Reduce strain on the tendon by supporting the arch. Do not re-form a collapsed arch, but prevent further collapse and reduce pain.
PTTD ankle brace:
- Supportive device worn around the ankle and foot that helps reduce strain on the damaged posterior tibial tendon, supports the arch, relieves pain, and makes walking easier.
- Better for Stage II.
4. NSAIDs and Medications
They can be used to reduce pain and swelling, but they cure the underlying tendon problem.
When Is Surgery Needed?
Surgery may be considered when conservative treatment fails or when deformity becomes rigid that is it cannot be manually corrected by doctors..
Procedures include:
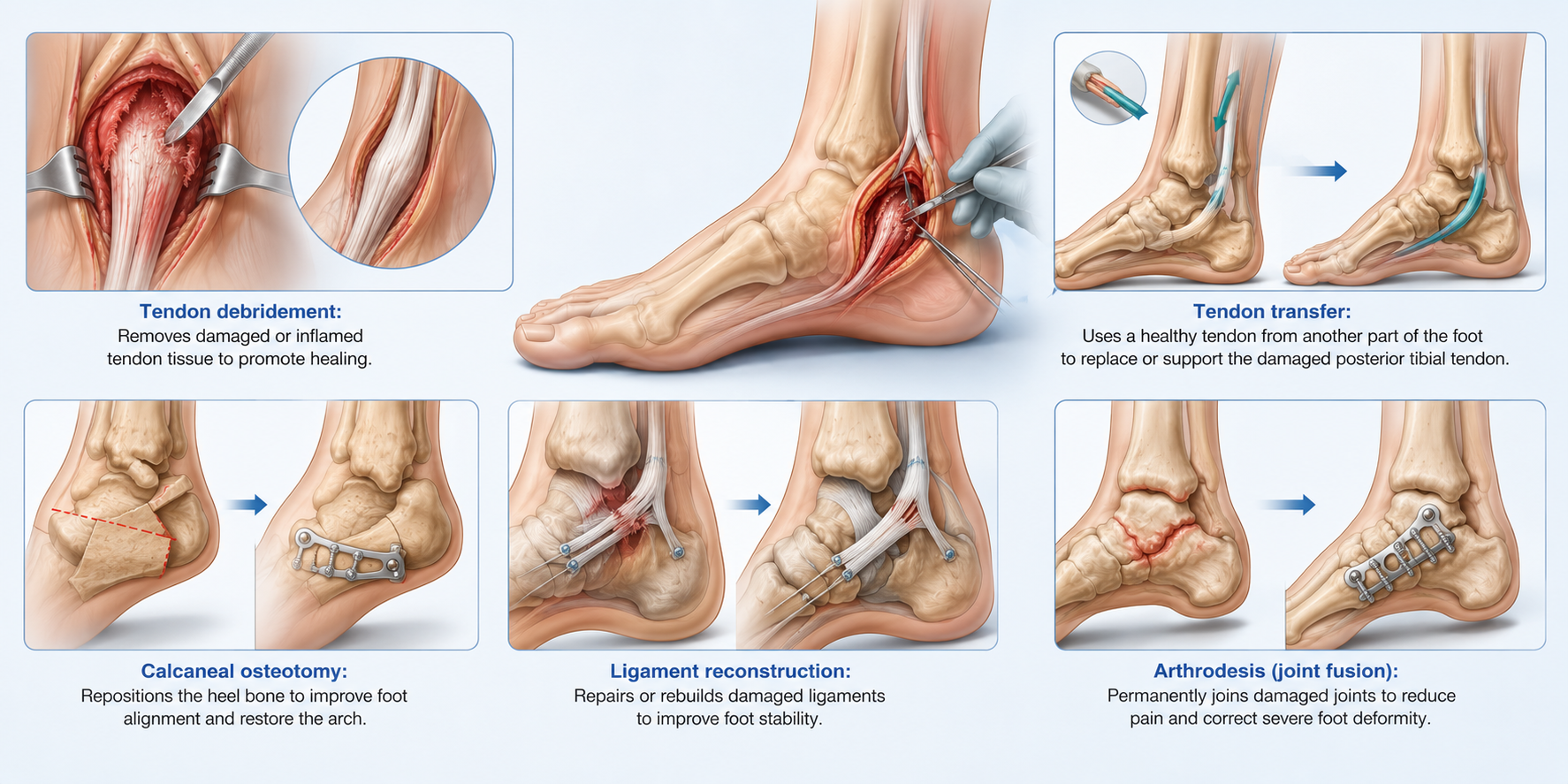
The choice depends on disease stage and patient activity level.
PTTD Exercises
Patients are advised to perform PTTD exercises at home as suggested by their doctors to improve recovery and restore activity.
Phase 1: Weeks 1–3
This phase aims at pain control and activation.
Toe curls: Sit with a towel on the floor. Use your toes to scrunch it toward you. 3 sets of 15.
Calf raises (double leg, flat ground): Rise slowly onto both toes, hold 2 seconds, lower for 4 seconds. 3 sets of 15.
Seated arch lifts: Sit with your feet flat. Lift the arch off the floor without curling toes. Hold 5 seconds. Repeat 10 times.
Phase 2: Weeks 4–8
Strengthening exercises are an important part of recovering from PTTD. One type, called eccentric exercises, involves slowly lowering your foot or heel while keeping the muscle under tension.
These exercises can help strengthen the tendon, reduce pain, and improve foot function when performed as part of a guided rehabilitation program.
Single-leg eccentric heel lowering: Stand on the edge of a step on one foot. Rise onto toes using both feet. Shift weight to the affected foot. Slowly lower your heel below the step over 5–8 seconds. Use both feet to rise again.
Resistance band inversions: Sit on the floor, loop a band around your foot. Slowly pull your foot inward against resistance.
Single-leg balance: Stand on the affected foot for 30 seconds, progress to 60 seconds, then on an unstable surface like a folded towel.
Phase 3: Weeks 9–12
This phase aims at functional strengthening exercises.
Single-leg calf raises: Progress to complete single-leg raises from a flat surface.
Step-down exercise: Step slowly off a 15cm step onto the affected leg, controlling the descent.
Walking lunges with arch engagement: Focus on maintaining the arch of your foot throughout each step.
Can PTTD Heal Without Surgery?
Yes if diagnosed in early stages that is Stage I or early Stage II improve without surgery with conservative treatment which includes:
- Orthotics
- Bracing
- Weight management
- Progressive strengthening exercises
- Activity modification
Complications of Untreated PTTD
If left untreated, PTTD can progressively damage the foot and ankle, leading to:
- The arch gradually collapses leading to an acquired flat foot which makes walking difficult.
- Posterior tibial tendon may tear completely leading to loss of arch support
- Pain may become persistent and limit daily activities.
- Posterior tibial tendon support loss makes the ankle feel weak or unstable, thus walking difficult.
- Abnormal foot alignment increases stress on the joints, leading to arthritis in the foot and ankle over time.
- Everyday activities, work, exercise and in later stages even walking may become difficult.
Prevention of PTTD

Recovery Timeline from PTTD
| Stage | Approximate Recovery |
|---|---|
| Mild tendonitis | 6–8 weeks |
| Stage I PTTD | Approximately 3 months |
| Stage II PTTD | 3–6 months |
| Surgical treatment | 6–12 months |
People with Stage I and Stage II PTTD can return to activities like running with the right footwear, orthotic support, and a gradual return protocol. This typically begins around 3–4 months into recovery, starting with walking intervals, progressing to jogging on soft surfaces under proper supervision and guidance by the doctor and physiotherapist.
Key Takeaway's
- PTTD is a progressive condition that weakens the tendon responsible for supporting the arch of the foot, potentially leading to adult-acquired flatfoot.
- Early symptoms include pain and swelling along the inside of the ankle, especially after walking, running, or standing for long periods.
- Early diagnosis and conservative treatment, such as rest, orthotics, physical therapy, and strengthening exercises, can help relieve symptoms and slow disease progression.
- Surgery may be recommended for advanced cases when conservative treatments fail or when the foot deformity becomes rigid.
- Early identification and treatment are the main strategies to better recovery from PTTD

Not every foot pain is caused by tendon damage, sometimes a hidden hairline fracture may be the real culprit. Learn how to tell the difference.
Frequently Asked Questions
Is PTTD the same as flat feet?
No. PTTD is a common cause of adult-acquired flatfoot, but not everyone with flat feet has PTTD.
Can walking make PTTD worse?
Yes. Prolonged walking may aggravate symptoms, particularly during flare-ups.
Is PTTD permanent?
Early stages can improve significantly. Advanced stages may result in irreversible structural changes.
Does MRI always diagnose PTTD?
MRI is useful but diagnosis is primarily based on clinical findings. MRI can help detect inflammation, degeneration, tears, or ruptured tendon in PTTD.
What shoes are best for PTTD?
Supportive shoes with firm arch support, a stable heel support, and cushioned soles are generally recommended for PTTD patients. Custom orthotics or ankle braces may also be advised to reduce stress on the tendon.
Reference's
- American Academy of Orthopaedic Surgeons. Posterior Tibial Tendon Dysfunction (Progressive Collapsing Foot Deformity).
- American Orthopaedic Foot & Ankle Society. Progressive Collapsing Foot Deformity (Adult Acquired Flatfoot).
- Kulig K, Reischl SF, Pomrantz AB, et al. Nonsurgical management of posterior tibial tendon dysfunction with orthoses and resistive exercise: a randomized controlled trial. Physical Therapy. 2009;89(1):26–37.








Member discussion