


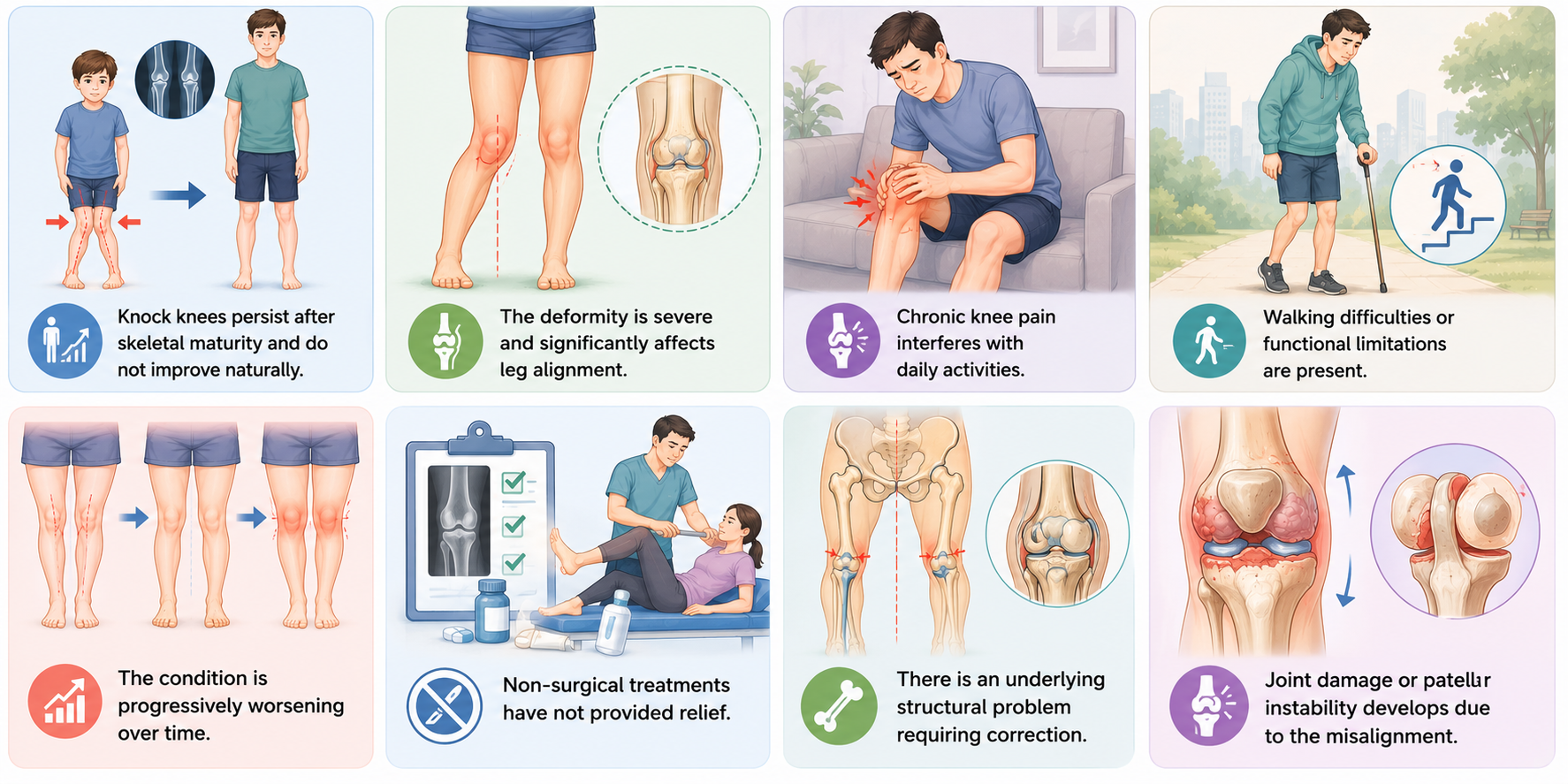
Knock knees, technically called genu valgum, is where a person's knees bend inwards and touch each other, while their ankles remain wide apart when standing up. Knock knees are quite normal when a child is very young, and usually correct themselves. If knock knees persist after the age of about seven or they start to become more severe, or they give the person pain when walking, they may need treatment for an underlying condition.
It's important to be knowledgeable on the various causes of genu valgum and its symptoms, as well as treatment options available to manage joint health. Treatments vary from lifestyle changes and physiotherapy to surgical correction in serious cases, but the optimal treatment will vary depending on age and severity of symptoms. Here you will find a full guide covering everything you want to know about knock knees, such as what they are, when they are normal, diagnosis, treatment and when to seek professional help.
What Are Knock Knees? Understanding Genu Valgum
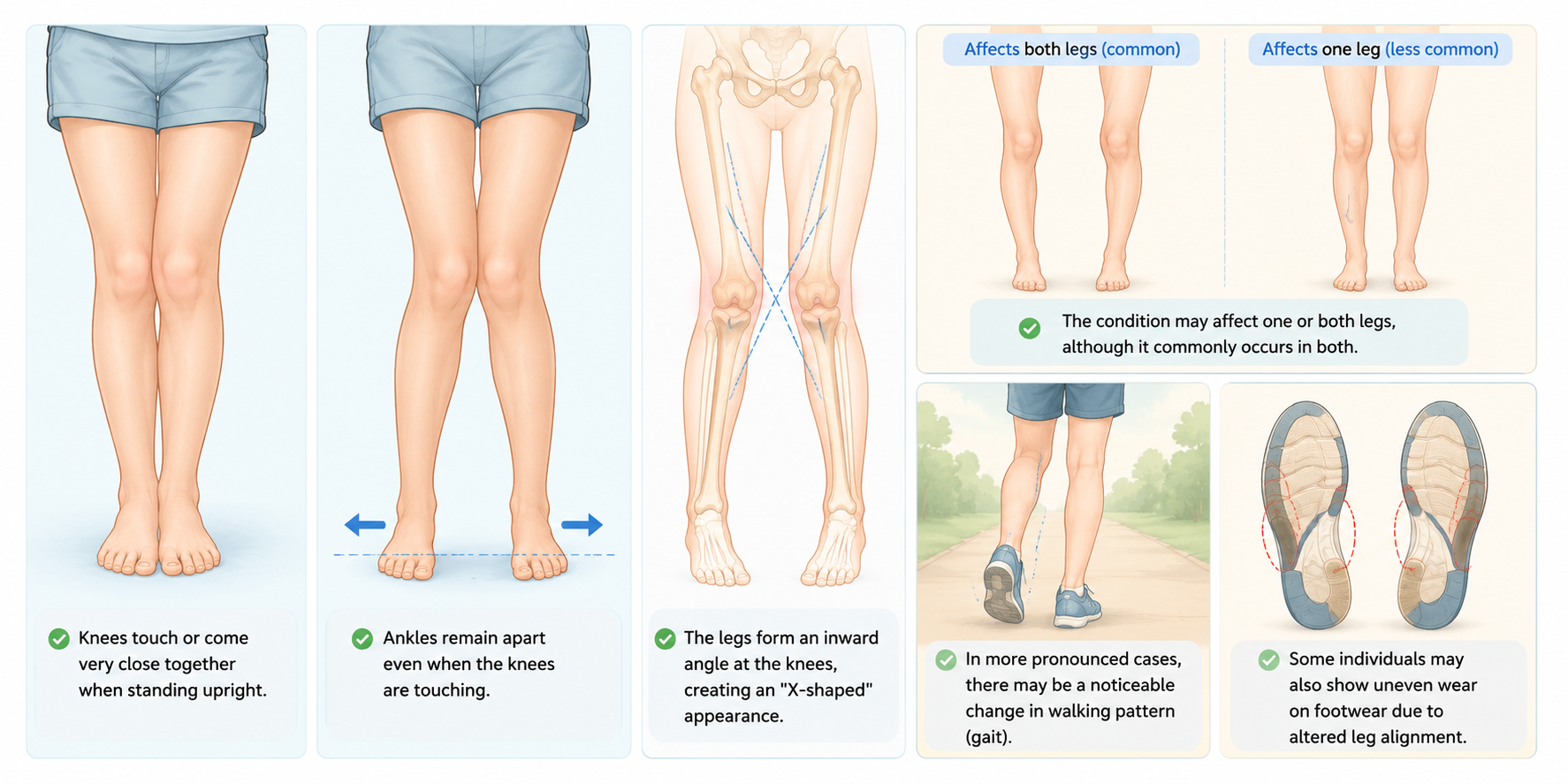
Knock knees, also medically known as genu valgum, occurs when an individual's knees angle inward and touch one another while standing with their legs relatively straight. Their ankles, however are not touching and the legs angle outward below the knees.
Visual Characteristics of Knock Knees (Genu Valgum) :
Key Measurement :
The intermalleolar distance the gap between the inner ankles when the knees are touching is commonly used to assess the severity of knock knees (genu valgum).
Normal vs. abnormal:
In children between the ages of two to seven,knock kneesare frequently normal and many resolve with age without intervention. If the knee knock becomes worse, or appears or progresses after the age of seven or eight, it should be assessed by a health professional.
Types of Knock Knees: Physiological vs. Pathological
Not all cases of knock knees are the same. While physiological knock knees are a normal part of a child's growth and usually correct themselves over time, pathological knock knees result from an underlying condition and may require medical attention. Understanding the differences can help determine when reassurance is enough and when professional evaluation is needed.
| Feature | Physiological Knock Knees | Pathological Knock Knees |
|---|---|---|
| Definition | A normal stage of childhood growth and development. | An abnormal condition caused by an underlying medical issue. |
| Typical Age | Common between 2–7 years, peaking around 3–4 years of age. | Can occur at any age and may persist beyond 7–8 years. |
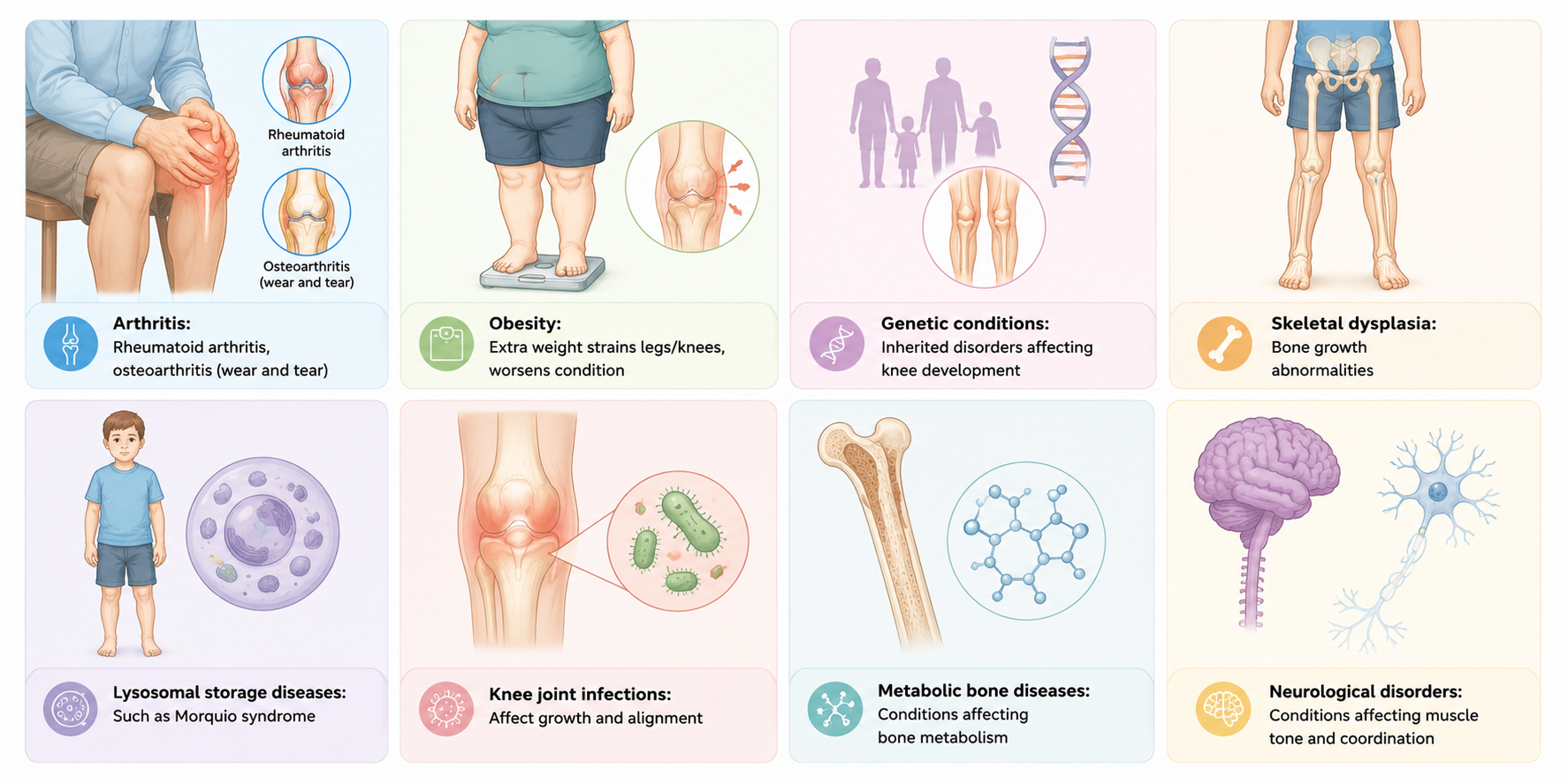
| Cause | Natural changes in leg alignment during growth. | Conditions such as rickets, skeletal dysplasia, obesity, growth plate injuries, infections, or metabolic bone disorders. |
| Symmetry | Usually affects both legs equally. | May affect one leg more than the other (asymmetrical). |
| Progression | Gradually improves on its own with age. | May persist, worsen, or develop suddenly over time. |
| Pain | Typically painless. | May be associated with knee pain, hip pain, or discomfort while walking. |
| Walking Pattern | Normal gait with little or no functional limitation. | May cause limping, altered gait, frequent tripping, or difficulty running. |
| Growth and Development | Child usually has normal growth and development. | May be accompanied by short stature, delayed growth, or other skeletal abnormalities. |
| Need for Investigations | Usually not required unless the condition is severe or persistent. | Often requires X-rays, blood tests, and further medical evaluation to identify the underlying cause. |
| Treatment Approach | Observation and reassurance; no specific treatment is usually needed. | Focuses on treating the underlying cause and may include nutritional therapy, physical therapy, guided growth surgery, or osteotomy. |
| Prognosis | Excellent; most cases resolve naturally by age 7–8 years. | Depends on the underlying condition and the timeliness of treatment. |
| When to Seek Medical Advice | If knock knees persist beyond age 7–8 years or become more pronounced. | Prompt evaluation is recommended, especially if there is pain, asymmetry, worsening deformity, limping, or associated growth concerns. |
Common Causes of Knock Knees
Normal Developmental Causes :
- Physiological growth pattern: Mild knock knees commonly develop as part of normal skeletal growth in children.
- Typical age-related alignment changes: Genu valgum is often most noticeable between 2 and 7 years of age.
- Natural correction with growth: For most children, leg alignment corrects on its own by the age of 7-8 without intervention.
- Symmetrical involvement: Developmental knock knees generally involve equal involvement of both legs and is painless and doesn't affect function.
Normal leg alignment by age :
- Birth to 18 months: bow legs
- Ages 2–4 years: knock knees peak
- Ages 7–8 years: alignment usually improves
Genetic/Family History of Genu Valgum :
- Inherited tendency : Knock knees can run in families, increasing the likelihood of developing genu valgum.
- Shared bone structure : Children may inherit leg alignment patterns similar to their parents or close relatives.
- Not always problematic : Mild familial genu valgum may not cause symptoms or require treatment.
- Monitor persistent cases : A family history combined with worsening deformity, pain, or functional limitations may warrant medical evaluation.
Nutritional Deficiencies
| Deficiency | Condition Caused | Impact on Knock Knees (Genu Valgum) |
|---|---|---|
| Vitamin D | Rickets | Softens growing bones, leading to abnormal leg alignment and knock knees. |
| Calcium | Poor bone mineralization | Weakens bones and may contribute to skeletal deformities. |
| Phosphorus | Impaired bone development | Affects bone strength and proper growth, increasing the risk of genu valgum. |
| Vitamin C | Scurvy (rare) | Impairs collagen formation, affecting bone and connective tissue health. |
| Protein | Protein-energy malnutrition | Can interfere with normal growth and skeletal development in children. |
Knock Knees vs. Bow Legs: Understanding the Difference :
Knock knees, more formally called genu valgum, and bow legs, or genu varum, differ in the way that the legs are angled. The table below explains these differences.
| Feature | Knock Knees (Genu Valgum) | Bow Legs (Genu Varum) |
|---|---|---|
| Leg appearance | Knees touch while the ankles remain apart. | Ankles touch while the knees remain apart. |
| Direction of alignment | Lower legs angle outward below the knees, creating an inward knee position. | Lower legs angle inward below the knees, creating an outward bowing appearance. |
| Overall shape | "X-shaped" appearance of the legs. | "O-shaped" appearance of the legs. |
| Common age of occurrence | Typically seen between 2–7 years of age as part of normal development. | Common in infants and toddlers younger than 2 years. |
| Natural course | Often resolves spontaneously by 7–8 years of age. | Usually improves naturally by 18–24 months of age. |
| Weight distribution | May increase stress on the outer compartment of the knee. | May increase stress on the inner compartment of the knee. |
| Potential complications | Knee pain, gait abnormalities, and patellar instability in severe cases. | Joint pain, uneven wear of the knee joint, and mobility issues if persistent. |
| When to seek medical advice | If persistent after 7–8 years, worsening, asymmetrical, or associated with pain. | If persistent beyond 2 years, worsening, asymmetrical, or associated with pain. |
Medical Conditions :
Trauma and Injury :
- Growth plate injuries: Damage to the growth plate near the knee can affect normal bone growth and lead to knock knees.
- Poorly healed fractures: Fractures of the thighbone (femur) or shinbone (tibia) that heal incorrectly may alter leg alignment.
- Knee trauma: Significant injuries involving the knee joint can contribute to the development of genu valgum.
- Post-traumatic deformity: Uneven bone growth after an injury may cause one or both legs to angle inward over time.
Pregnancy-Related Factors :
- Weight gain during pregnancy increases knee stress : The additional body weight during pregnancy places extra pressure on the knee joints, which may affect leg alignment and worsen existing symptoms.
- Hormonal changes (relaxin) affect ligament flexibility : Pregnancy hormones, particularly relaxin, loosen ligaments to prepare the body for childbirth, potentially reducing joint stability around the knees.
- Post-pregnancy weight may not return, leading to persistent knock knees : Retaining excess weight after delivery can continue to place strain on the knees and contribute to ongoing alignment issues.
- Worsening of pre-existing knock knees during pregnancy : Women with pre-existing genu valgum may notice increased knee discomfort or a temporary worsening of the condition due to pregnancy-related physical changes.
Symptoms and Signs of Knock Knees :
- Knees touch or rub together while standing with the ankles apart.
- Noticeable gap between the ankles when the knees are touching.
- Inward angulation of the legs, creating an "X-shaped" appearance.
- Altered walking pattern (gait), such as awkward or waddling movement.
- Frequent tripping or clumsiness, especially in children.
- Uneven wear on shoes due to changes in leg alignment.
- Difficulty keeping the feet together while standing straight.
- One leg may appear more affected than the other in some cases.
- Reduced balance or coordination during physical activities.
- Visible worsening of leg alignment over time, particularly after the expected age of correction.
Functional Symptoms :
| Symptom | Description |
|---|---|
| Knee pain | Increased pressure on the inner or outer part of the knee joint due to misalignment. |
| Walking difficulties | Altered gait patterns, limping, or balance problems that affect normal walking. |
| Leg fatigue | Extra strain on the muscles surrounding the knees, leading to tiredness during activity. |
| Hip or ankle pain | Occasional discomfort in the hips, ankles, feet, or knees caused by abnormal weight distribution. |
| Out-toed gait | Rarely, the feet may point outward as valgus alignment becomes more pronounced. |
| Lateral patella subluxation | Rare displacement of the kneecap toward the outer side of the knee. |
| Difficulty running | Reduced speed, endurance, or participation in sports and other physical activities. |
| Clumsiness | Increased stumbling, tripping, or falling, particularly in children. |
When to See a Doctor :

How Knock Knees Are Diagnosed :
Physical Examination :
- Assessment of leg alignment while standing and walking.
- Measurement of the intermalleolar distance (gap between the inner ankles when the knees touch).
- Evaluation of gait pattern to identify limping or balance issues.
- Examination of knee range of motion and joint stability.
- Assessment for pain, tenderness, or swelling around the knees.
- Comparison of both legs to check for asymmetry or unequal involvement.
- Measurement of height and weight, especially in children, to assess growth patterns.
- Review of medical and family history for previous injuries, nutritional deficiencies, or inherited conditions.
- Assessment of hip, ankle, and foot alignment to identify associated abnormalities.
- Monitoring progression over time through follow-up examinations when necessary.
Imaging Tests :
- X-rays: Used to inspect bones for any changes, rule out possible disease processes
- MRI: Shows better details of bones
- Measure at angle of bone growth (if >20 degrees, a procedure may be necessary)
- CT scan may be necessary for unusual fractures
- Bone scan may be useful if there is suspicion of osteoporosis
Laboratory Tests :
- Blood tests- rule out vitamin deficiencies and metabolic problems
- test vitamin D levels, calcium levels
- check inflammatory markers if arthritis is suspected
- genetic testing if there is a suspected inherited disease
Treatment Options for Knock Knees :
When No Treatment Is Needed :
- The child is between 2–7 years old with typical developmental knock knees.
- Both legs are equally affected (symmetrical alignment).
- There is no pain or difficulty walking.
- The condition is stable or gradually improving with growth.
- No underlying medical condition is suspected.
- Regular monitoring by a healthcare provider shows normal progression.
Treating Underlying Causes :
| Cause | Treatment |
|---|---|
| Vitamin D deficiency (Rickets) | Vitamin D and calcium supplementation, along with dietary modifications and medical follow-up. |
| Obesity | Weight management through a balanced diet, regular physical activity, and lifestyle changes. |
| Previous fractures or growth plate injuries | Orthopedic evaluation and treatment, which may include monitoring or corrective procedures. |
| Bone disorders (e.g., skeletal dysplasia) | Specialist management tailored to the specific underlying condition. |
| Arthritis or inflammatory joint conditions | Medications, physiotherapy, and treatment directed at controlling inflammation. |
| Metabolic bone diseases | Medical management to correct nutritional or hormonal imbalances affecting bone health. |
| Infections affecting bone growth | Appropriate antimicrobial therapy and orthopedic follow-up if needed. |
Exercise and Physical Therapy :
Exercise strengthens leg muscles, improves posture/balance in young adults; research insufficient for children.
Recommended exercises (consult doctor before starting):
- Side lunges: 10-12 reps per leg
- Stand hip-width apart, arms at chest
- Step sideways, bend knee, push hip back
- Return to neutral position
- Lying abduction: 10-12 reps per leg
- Lie on side, legs stacked
- Lift leg at 45-degree angle, hold 1 second
- Lower slowly
- Wall squat: Hold 5-10 seconds, increase duration
- Stand against wall, feet shoulder-width
- Squat to ≤90 degrees
- Keep abdominal muscles contracted
- Optional: add resistance band around knees
- Additional exercises: Stretches that reposition knees and relieve pain
Exercise precautions :
- Avoid high-impact activities if they worsen knee pain.
- Stop exercising if you experience significant discomfort.
- Use proper technique during workouts and stretching exercises.
- Wear supportive footwear to improve alignment and stability.
- Increase exercise intensity gradually to prevent overloading the joints.
- Focus on low-impact activities such as swimming or cycling when needed.
- Perform exercises under professional guidance if symptoms are severe.
- Warm up and cool down properly before and after physical activity.
Weight Management :
- Weight loss recommended for overweight individuals
- Extra weight strains legs/knees, worsens condition
- Combine diet + exercise for weight loss
- Substitute high-impact for low-impact exercise
- Target 5-10% weight loss for significant improvement
- Monitor progress with regular weigh-ins
Orthotics and Braces
- Orthotics: shoe inserts may help improve foot alignment and walking comfort.
- races/splints: Help bones grow correctly in children
- Guided growth plates: For children <10 with 15-20° angle
- Plates, screws, or staples implanted in bone
- Minimal-incision procedure
- Metal plate removed after alignment achieved
- Night splints: For mild cases in children
When surgery is needed :
| Procedure | Age Group | Description |
|---|---|---|
| Guided Growth Surgery (Hemiepiphysiodesis) | Children | A small metal plate or screw is inserted near the growth plate to gradually guide bone growth and improve alignment. |
| Femoral Alignment Surgery | Adolescents | Corrects the angle of the femur (thigh bone) to restore normal leg alignment. |
| Distal Femoral Osteotomy | Older teens, adults | The lower part of the femur is cut and repositioned to correct severe valgus deformity. |
| Tibial Osteotomy | Older teens, adults | The tibia (shin bone) is surgically realigned when the deformity originates from the lower leg. |
| Osteotomy | Adults, older teens | The surgeon cuts and realigns the bone, securing it with plates and screws to correct the deformity. |
| Knee Replacement | Rare, severe cases | An artificial knee joint is used to replace a damaged joint and correct genu valgum associated with advanced arthritis. |
| Corrective Limb Reconstruction | Selected severe cases | Advanced procedures are performed to address complex deformities and restore limb alignment. |
| External Fixation (Gradual Correction) | Complex or severe cases | An external frame is used to slowly adjust bone alignment over time, particularly in challenging deformities. |
Diet and Nutrition for Bone Health :
Essential Nutrients :
- Vitamin D: Essential for strong bone development; get from sun exposure + diet
- Calcium: Critical for bone strength; rich calcium diet recommended
- Protein: Supports muscle growth and joint stability
- Phosphorus: Works with calcium for bone health
- Magnesium: Supports bone structure
- Vitamin K: Important for bone mineralization
Recommended Foods :
- Anti-inflammatory foods: berries, leafy greens
- Sun exposure: Main source of vitamin D (15-30 min daily)
- Balanced diet for overall bone/joint health
- Calcium-rich foods: dairy, leafy greens, fortified foods
- Vitamin D foods: fish, eggs, fortified milk
- Protein sources: lean meat, fish, eggs, legumes
Prevention Through Nutrition :
- Early nutrition: Adequate calcium + vitamin D in childhood prevents rickets-related genu valgum
- Sun exposure: 15-30 minutes daily for vitamin D
- Infant feeding: Breastfeeding provides optimal vitamin D initially
- Supplement guidelines: Vitamin D supplements for infants if sun exposure limited
- Cultural considerations: In India, sun avoidance practices may increase rickets risk
Lifestyle Changes to Manage Knock Knees :
- Maintain a healthy weight to reduce pressure on the knees.
- Choose low-impact activities such as walking, swimming, or cycling.
- Perform strengthening exercises for the hips and leg muscles.
- Eat a balanced diet rich in calcium and vitamin D.
- Wear supportive footwear for better comfort and stability.
- Avoid activities that increase knee pain or strain.
- Follow your physiotherapy plan and attend regular check-ups if advised.
Age-Specific Considerations
| Age Group | Key Considerations for Knock Knees (Genu Valgum) |
|---|---|
| Infants and Toddlers (0–2 years) |
|
| Preschool Children (3–5 years) |
|
| School-Age Children (6–10 years) |
|
| Adolescents (11–17 years) |
|
| Adults (18+ years) |
|
| Older Adults (65+ years) |
|
Mental Health and Quality of Life Impact :
Self-Esteem, Social Impact, and Lifestyle Considerations : Knock knees can affect self-esteem and body image, particularly in children and adolescents who may feel self-conscious about the appearance of their legs. Peer comments or teasing can sometimes impact confidence, leading some individuals to avoid activities that expose the legs, such as swimming or certain sports. This may contribute to social anxiety in group settings. Encouraging positive self-talk, open communication, and strong parental support can help improve coping and self-confidence. From a practical perspective, some people may prefer clothing styles such as pants or leggings that make them feel more comfortable, while supportive footwear with good arch support and, when recommended, custom orthotics can help enhance comfort and stability.
Prevention Strategies
Early Childhood Prevention :
- Sun exposure: 15-30 minutes daily for vitamin D
- Breastfeeding: Provides optimal nutrition initially
- Vitamin D supplements: For infants with limited sun exposure
- Avoid W-sitting: Can worsen leg alignment
- Proper nutrition: Calcium + vitamin D rich diet
Weight Management Prevention :
- Prevent childhood obesity
- Healthy eating habits from early age
- Regular physical activity
- Monitor weight gain during pregnancy
Lifestyle Prevention :
- Regular exercise for bone strength
- Avoid prolonged sitting in poor positions
- Wear supportive footwear
- Maintain good posture
Key Takeaways
- Knock knees are often a normal stage of childhood growth.
- Most physiological cases resolve naturally by age 7–8 years.
- Persistent, painful, worsening, or asymmetrical knock knees should be evaluated by a healthcare professional.
- Early diagnosis helps identify treatable underlying causes.
- Treatment ranges from observation and lifestyle modifications to surgical correction in severe cases.
Conclusion :
Most children with knock knees naturally grow out of the condition by age 7-8 without treatment. However, if knock knees persist beyond age 8, appear in adulthood, affect only one leg, or cause pain, consult an orthopedic specialist to identify underlying causes like vitamin D deficiency or arthritis. For those who don't resolve naturally, exercises, weight management, orthotics, and proper nutrition (vitamin D + calcium) often provide relief without surgery. Prevention through adequate sun exposure, healthy weight, and good nutrition is key. In India, special attention to vitamin D deficiency is important due to cultural sun avoidance. With proper diagnosis and treatment, most people achieve excellent outcomes and maintain normal quality of life.

As knock knees alter weight distribution across the legs, the knees may become more prone to hyperextension.
Frequently Asked Questions :
Can knock knees be corrected without surgery?
Yes, most children outgrow them naturally. For adults/older children, exercises, stretches, weight loss, and orthotics often provide relief without surgery.
At what age should I worry about my child's knock knees?
Consult a doctor if: before age 2, after age 8, only one leg affected, gap >10 cm at age 4, pain present, or walking problems
Do exercises actually fix knock knees?
Exercise strengthens leg muscles and improves posture/balance in young adults. Research insufficient to confirm correction in children.
Will knock knees cause knee problems later in life?
Untreated severe knock knees can lead to joint pain, early arthritis, and long-term knee issues due to excessive force on knees.
What's the difference between physiological and pathological knock knees?
Physiological = normal development (ages 3-5, resolves by 7-8). Pathological = severe, persists beyond age 8, or develops in adulthood, often with underlying cause.
Can I prevent knock knees in my child?
Ensure adequate vitamin D (sun exposure + supplements), calcium-rich diet, prevent obesity, avoid W-sitting, and monitor for early signs
How long does it take to see results from exercises?
Typically 3-6 months for noticeable improvement; consistent daily exercise required
Is exercise enough for adult knock knees?
For adults, exercises alone may not fully correct alignment but can reduce pain and improve function. Weight management + orthotics often needed







Member discussion